What is a Hip Flexor Strain?
Hip flexor strain is also known as Iliopsoas syndrome and is a common sports injury (3,5% of all sports injuries). It is the pain that appears on the front side of the hip and pelvis and is caused by sudden swinging or repetitive flexion in the hip joint. The muscle is partially attached to the lumbosacral spine and on the other side is attached to the femur, thigh bone.
Mechanism of movement and anatomy
The flexion movements extend the iliopsoas muscle and induce inflammation. Another muscle that may be responsible is the Rectus femoris muscle. These two muscles are responsible for bringing the leg to the front and flexion in the hip and for bringing the knee to the chest, and they need to be strong and durable because they elevate the weight of the whole leg.

When the muscles and their tendons extend over the limits, they become damaged and injured. The exertion of the muscles is larger if the movements involve kicking the ball. Mostly, these injuries occur in jumpers, runners, ballet dancers etc.
Risk Factors
Risk factors are some immuno-compromising conditions and some professional errors, such as not warming up, not performing the movements properly, weak muscles, poor posture, fatigue, joint stiffness or previous injuries with protection of the injured segment in lumbosacral and leg region etc. (1)
Degrees of injury
There are three degrees of the muscle damage:
- 1st degree injury – mild injury, walking is enabled. Some fibres are injured.
- 2nd degree injury – some fibres are damaged which results in weakness of the muscle and moderate pain. This is the commonest degree of injury.
- 3rd degree injury – partial or a total rupture to the muscle. (2)
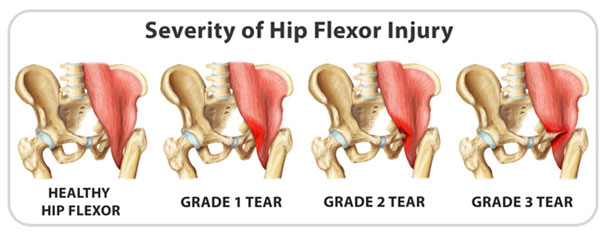
Figure 1 Degrees of hip flexor injury (3)
A person may experience this pain from time to time due to continuous improper movements of the hip and Psoas muscle, causing chronical hip flexor pain. These muscles are actually under a lot of tension in general, even in people who sit too much during the day. In this case, these muscles are constantly contracted which may lead to contractures and problems with moving and standing up.
Signs and symptoms
The pain appears immediately after an injury or with some simple tasks like tying the shoes or bending the knees, which leads a person to the doctor’s office. The pain is sudden, intensive and sharp or with pulling sensation, and in the front side of the hip, or sometimes in the lower part of back. The pain may also be mild and in form of slight discomfort or can be in form of cramps and spasms.
Sometimes the pain is in the groin which may raise the question of whether the injury is in the adductor muscles of the leg. Pain spreads down through the whole leg. Pain is provoked when the leg is flexed towards the chest.
A person may feel stiffness in the muscles and tenderness on palpation. If there is a complete rupture to the muscles in extreme cases, there could be signs of haematoma and swelling in the inguinal area at the lowest point. A person has a difficulty in gait and limps. If the swelling and haematoma progress, they may compress the nerves and veins causing more problems, but this happens rarely.
Diagnosis
After taking a history, and receiving the information about the type of the injury, the doctor will suspect the injury to the Iliopsoas muscle. Rectus femoris muscle is much rarer damaged than Iliopsoas muscle. In adolescents, there is a high risk of avulsion fracture, so there are sometimes indications to do an X ray to exclude such event. Avulsion fracture is a frequent event among young sports, when the tendon is strongly pulled, in such strength that it pulls out a part of the bone, and induces a fracture.
Additional procedures may sometimes be indicated: MRI, CT or X rays, and ultrasound may be useful to exclude some other conditions such as abdominal hernia or lumbal disc hernia. (2)
Treatment
Initial treatment
In the acute phase, in the first 24-72 hours, when there is pain and limited movements, there is a need for ice application, rest and elevation of legs to prevent swelling. Ice is not applied directly on skin, but rather wrapped in a towel, for 15 minutes 3-4 times a day.
Taking analgesics, usually NSAIDs will help in pain relief. It is also important to apply some compressive bandages around the hip, or in form of shorts, to prevent swelling, but they shouldn’t be bound tight, because that would compromise the circulation.
The PRICE method (protection, rest, icing, compression and elevation) is crucial in promoting the healing processes and prevention of complications, especially if there is a complete rupture of the muscle. (4)
Second phase-exercises
Exercises are useful after the acute phase and when the pain vanishes or is significantly lowered. Exercises include stretching and strengthening the muscles to improve circulation and promote healing.
Exercising too early may have opposite effect and delayed recovery. (5) Exercises include flexion and exstension in the hip joint. Isometric contractions are used in the first phase of recovery, to prevent further damage and promote healing.
Isometric contractions include stretching the muscles without moving the legs, for example by pushing against a hard surface. This way, ther muscle fibres contract minimally and gradually which is necessary in healing process. (6)
Other methods include sports massages, electrotherapy, aquatic rehabilitation in the swimming pools, biomechanical correction, education and prevention. (2)
Comeback Strategies & Prognosis
It is important to keep the joint moving and reduce the chance for a frozen joint, but also it is important to evaluate when is the right time to begin with physical kinesitherapy, which is something that a sports medicine specialist will have to evaluate.
The pain and restricted movement may last for up to couple of months which may have effect on the sports results and performance. Those with mild injuries will recover in 3 weeks, and when the injury is more severe, there is a need for rest in duration of 6-8 weeks. In complete ruptures, there is a need for a longer rest and restriction from sports.
Works Cited
- Psoas syndrome. Cleveland Clinic. [Online] 2015. [Cited: 3 19, 2017.] http://my.clevelandclinic.org/health/articles/psoas-syndrome.
- Hip Flexor Strain. Physio Advisor. [Online] [Cited: 3 19, 2017.] https://www.physioadvisor.com.au/injuries/hip-groin/hip-flexor-strain/.
- SPORTS MEDICINE: Hip flexor strain – a long term problem for hockey players. gohockey. [Online] [Cited: 3 19, 2017.] http://gohockey.com/sports-medicine-hip-flexor-strain-a-long-term-problem-for-hockey-players/.
- Hip Flexor Strain. Athletes treating athletes. [Online] 2013. [Cited: 3 19, 2017.] http://athletestreatingathletes.com/hip-flexor-strain/.
- M., Zehr. How to Treat a Hip Flexor Strain. Live Strong. [Online] 2015. [Cited: 3 19, 2017.] http://www.livestrong.com/article/342927-how-to-treat-a-hip-flexor-strain/.
- Hip Flexor Strain. Sports Injury Clinic. [Online] [Cited: 3 19, 2017.] http://www.sportsinjuryclinic.net/sport-injuries/hip-groin-pain/hip-strain.